Bicalutamide
比卡鲁胺
Bicalutamide
Oral
Bicalutamide is a potent non-steroidal androgen receptor (AR) antagonist originally developed for prostate cancer treatment. In transgender HRT, it is considered a last-resort antiandrogen — to be considered only when CPA, spironolactone, and GnRH agonists are all unavailable. WPATH SOC 8 explicitly does not recommend it for routine GAHT.
Pharmacology
Section titled “Pharmacology”Mechanism of Action
Section titled “Mechanism of Action”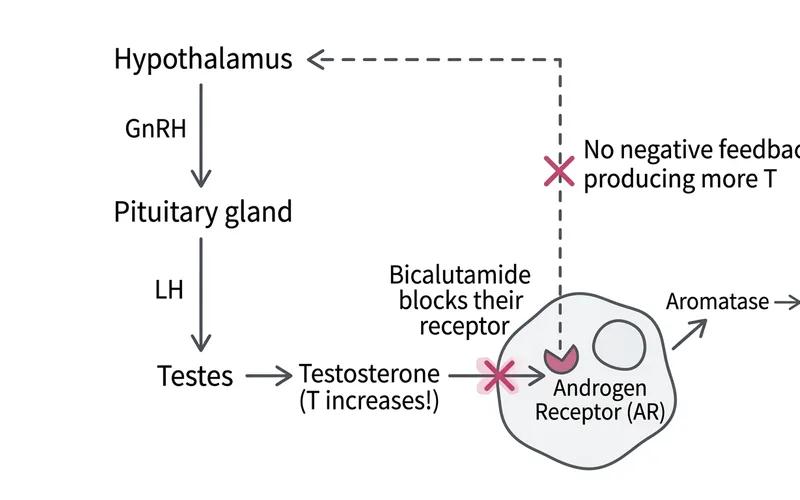
Bicalutamide is among the non-steroidal AR antagonists with the highest binding affinity currently in clinical use:
- Potent AR blockade (sole mechanism): Competitively blocks androgen receptors, preventing testosterone (T) and DHT from exerting biological effects
- Does not lower testosterone levels: Due to feedback mechanisms, T levels may actually rise
- No effect on the GnRH–LH/FSH axis: Does not suppress the hypothalamic–pituitary–gonadal axis
Pharmacokinetics
Section titled “Pharmacokinetics”- Oral bioavailability: Approximately 90%
- Steady-state half-life: 5–6 days — meaning a missed dose has minimal impact on plasma concentration, though frequent missed doses should still be avoided
- Time to peak concentration: Approximately 31 hours
- Time to steady state: Approximately 4 weeks
The Problem of Rising Testosterone Levels
Section titled “The Problem of Rising Testosterone Levels”This is a distinctive phenomenon when bicalutamide is used in GAHT [1] :
- Once bicalutamide blocks AR, the hypothalamus no longer senses androgen-mediated negative feedback
- The pituitary compensates by increasing LH secretion, stimulating the testes to produce more testosterone
- Serum testosterone levels may rise to 1.5–2× pre-treatment values
- While the biological effects of T are blocked, elevated T can be converted to estradiol via aromatase
- In prostate cancer patients, this testosterone rise sometimes leads to gynecomastia
Implications for transgender users: Although AR is blocked, elevated testosterone levels mean that if the drug is stopped or adherence drops, masculinizing effects may return rapidly.
Dosage Recommendations
Section titled “Dosage Recommendations”| Protocol | Dose | Notes | Source |
|---|---|---|---|
| Starting / Standard | 25 mg/day | Low dose used in the majority of transgender studies to date | Angus 2024; Burgener 2025 |
| Adjustment Range | 25–50 mg/day | Titrated based on clinical response | Neyman 2019 (50 mg); Angus 2024 (25 mg) |
| Absolute Maximum | 50 mg/day | Higher doses provide no additional benefit but increase hepatotoxicity risk | FDA label (prostate cancer combination therapy dose) |
Adverse Effects
Section titled “Adverse Effects”Hepatotoxicity (Most Important Risk)
Section titled “Hepatotoxicity (Most Important Risk)”Hepatotoxicity is the primary reason limiting bicalutamide’s use in GAHT [1] :
FDA label data (from prostate cancer clinical trials):
- Approximately 6% experienced transient asymptomatic ALT elevation
- Approximately 1% discontinued due to hepatitis or significant enzyme elevation
- Large 150 mg monotherapy trial (EPC, n=8,113): abnormal LFTs in 3.4% (vs. 1.9% placebo)
- At least 10 serious liver injury case reports have been published post-marketing, including 2 fatalities
Transgender population data (limited but informative):
- Neyman 2019: 23 adolescents, 50 mg/day, no clinically significant hepatotoxicity [2]
- Fuqua 2024: 40 adolescents in follow-up, 50 mg/day, no serious hepatic events [3]
- Angus 2024: 24 adults, 25 mg/day, 1 case of mild enzyme elevation (reversible) [4]
- Wilde 2024: 1 case report, 50 mg/day, hepatotoxicity developed (reversible upon discontinuation) [5]
These datasets remain too small in aggregate (approximately 170 cases) to rule out rare but serious hepatic injury.
Pulmonary Toxicity (Interstitial Lung Disease)
Section titled “Pulmonary Toxicity (Interstitial Lung Disease)”The FDA label includes a post-marketing warning for interstitial lung disease (ILD), including interstitial pneumonitis and pulmonary fibrosis, some of which have been fatal.
- Overall incidence is extremely low: approximately 0.01% (1/10,000), far lower than the related drug nilutamide (0.77%)
- Japanese pharmacovigilance data: Matsumoto 2020 analyzed the Japanese Adverse Drug Event Report database (JADER) and found a reporting odds ratio for bicalutamide-associated ILD of 9.2 (95% CI 7.9–10.6), with a median onset time of 50 days [6]
Breast Pain and Gynecomastia
Section titled “Breast Pain and Gynecomastia”- Bicalutamide commonly causes gynecomastia in prostate cancer patients
- In transgender users, this effect may be considered a desired outcome
- Breast tenderness is relatively common
Other Adverse Effects
Section titled “Other Adverse Effects”- Hot flashes (less frequent than with GnRH agonists)
- Gastrointestinal discomfort (nausea, diarrhea)
- Dry skin
Monitoring Requirements
Section titled “Monitoring Requirements”| Test | Frequency | Target / Alert Threshold | Action |
|---|---|---|---|
| Liver function (ALT/AST) | Baseline + monthly for the first 6 months → then every 3 months | ALT/AST ≤ upper limit of normal | >3× ULN: discontinue immediately and seek medical evaluation |
| Bilirubin | Concurrent with liver function tests | Normal range | Elevation indicates worsening hepatic injury |
| Testosterone (T) | Every 3–6 months | For reference only (T may be elevated) | Not a primary marker of treatment efficacy |
| Estradiol (E2) | Concurrent with testosterone | 100–200 pg/mL | Assess effectiveness of the combined regimen |
Appropriate Use Cases
Section titled “Appropriate Use Cases”Bicalutamide has a very limited role in GAHT [1] :
Consider only when all of the following conditions are met:
- CPA is unavailable (not marketed locally / intolerance / meningioma risk)
- Spironolactone is unavailable (renal impairment / hyperkalemia risk / insufficient effect)
- GnRH agonists are unavailable (financial / access barriers)
- Medical supervision and regular monitoring are in place
Contraindications:
- Pre-existing liver disease or abnormal liver function
- Currently using CPA or other hepatotoxic medications
- Unable to undergo regular liver function blood tests
Availability
Section titled “Availability”- Regulatory status: Bicalutamide is approved in mainland China (for prostate cancer treatment)
- Access: Can be prescribed through urology or oncology departments
- Brands: Casodex (originator) and domestic generics (e.g., Langyi)
- Cost: Originator approximately CNY 200–400/month; generics approximately CNY 50–150/month (50 mg tablets)
- Note: Most physicians are unfamiliar with its application in GAHT; obtaining a prescription may require framing the indication around prostate-related conditions
Brand Gallery
康士得 Casodex
- Maker
- 阿斯利康 (AstraZeneca)
- Spec
- 50mg × 28片
- Form
- 白色薄膜衣片
原研比卡鲁胺,价格较高
Calutide
- Maker
- Cipla
- Spec
- 50mg
- Form
- 白色薄膜衣片
Cipla 仿制比卡鲁胺,价格为原研的 1/5-1/10
Bicalox
- Maker
- 多种印度厂商
- Spec
- 50mg
- Form
- 白色薄膜衣片
印度仿制比卡鲁胺
Bicatero
- Maker
- Hetero
- Spec
- 50mg
- Form
- 白色薄膜衣片
Hetero 集团生产,全球仿制药大厂