GnRH Agonists
GnRH Agonists (GnRH 激动剂)
GnRH Agonists (Leuprorelin, Goserelin, Triptorelin, etc.)
Subcutaneous / Intramuscular Injection · Nasal Spray · Implant
GnRH Agonists are the most effective anti-androgen available, suppressing testosterone to castrate levels (< 50 ng/dL) by shutting down the hypothalamic-pituitary-gonadal axis. Both the Endocrine Society 2017 and WPATH SOC 8 recommend their use. When accessible, GnRH agonists are the ideal anti-androgen choice.
Pharmacology
Section titled “Pharmacology”How They Work
Section titled “How They Work”GnRH agonists act at a fundamentally different level than other anti-androgens — they target the upstream control center of hormone production [1] :
- Flare-Up Phase: For the first 1-2 weeks, the drug overstimulates pituitary GnRH receptors, causing a transient spike in LH/FSH and testosterone.
- Receptor Desensitization: Continuous stimulation causes pituitary GnRH receptors to downregulate and become unresponsive.
- Total Suppression: Within 2-4 weeks, LH/FSH output ceases, dropping T to castrate levels (< 50 ng/dL).
This mechanism suppresses T directly and reliably — without the hepatotoxicity risk of CPA or the hyperkalemia risk of spironolactone [2] .
T Suppression Compared to Other Anti-Androgens
Section titled “T Suppression Compared to Other Anti-Androgens”| Anti-Androgen | Mechanism | T Suppression | Main Limitation |
|---|---|---|---|
| GnRH Agonists | HPG axis shutdown | ~95% (< 50 ng/dL) | Extremely expensive; injection required |
| CPA 5-12.5mg | AR antagonism + progestogenic feedback | ~90% (female range) | Meningioma risk (≥25mg) |
| Spironolactone 100-200mg | Weak AR antagonism | ~30-50% (often insufficient) | Hyperkalemia; unreliable T suppression |
| Bicalutamide 50mg | Pure AR antagonism | T may increase | Hepatotoxicity; requires monitoring |
Available Formulations
Section titled “Available Formulations”Injectable Forms
Section titled “Injectable Forms”| Drug | Brand Names | Dose | Interval | Route | Self-Administration |
|---|---|---|---|---|---|
| Leuprorelin | Lupron / Eligard / Prostap | 3.75mg / 11.25mg / 22.5mg / 45mg | Monthly / 3-month / 6-month | SubQ or IM | Some SubQ forms can be self-injected |
| Goserelin | Zoladex | 3.6mg / 10.8mg | Monthly / 3-month | SubQ implant (abdomen) | Requires clinical administration (16G needle) |
| Triptorelin | Decapeptyl / Trelstar | 3.75mg / 11.25mg / 22.5mg | Monthly / 3-month / 6-month | IM injection | Requires clinical administration |
Non-Injectable Forms
Section titled “Non-Injectable Forms”| Drug | Brand | Form | Administration | Advantage | Limitation |
|---|---|---|---|---|---|
| Buserelin | Suprefact | Nasal spray | 2-3 sprays daily | No injection needed | Compliance burden (multiple daily doses) |
| Nafarelin | Synarel | Nasal spray | 2-3 sprays daily | Non-invasive; ~95% T reduction | Limited global supply |
| Histrelin | Supprelin LA | SubQ implant rod | Surgical insertion in upper arm; lasts 12 months | Once-yearly; best compliance | Very expensive; requires surgical insertion/removal |
Administration Guide
Section titled “Administration Guide”Subcutaneous Injection (Leuprorelin, etc.)
Section titled “Subcutaneous Injection (Leuprorelin, etc.)”Most GnRH agonists are administered via subcutaneous or intramuscular injection. Some formulations (e.g., leuprorelin SubQ) can be self-administered after nurse training [1] .
Injection Site Selection:
- Primary: Abdomen, approximately 5cm lateral to the navel (avoid 2cm around navel)
- Alternative: Anterior outer thigh, mid-section
- Rotation: Alternate sites each injection; maintain at least 3cm between injection points; avoid areas with lumps or bruising
Subcutaneous Injection Steps:
- Prepare: Wash hands. Bring refrigerated medication to room temperature (15-30 minutes). Check expiry date and solution appearance.
- Clean: Swab injection site with alcohol prep pad. Allow to air-dry completely.
- Pinch: Using your non-dominant hand, pinch a 2cm fold of skin.
- Insert: Insert needle at 45-90° angle quickly and firmly, burying the needle fully (1-2cm depth).
- Inject: Depress plunger slowly over ~30 seconds. Do not rush.
- Withdraw: Release skin, then withdraw needle swiftly. Press dry cotton ball on site for 15 seconds (do not rub).
- Dispose: Place needle in sharps container. Record date and injection site.
Indian GnRH Lyophilized Powder Reconstitution (Lupride Depot etc.)
Section titled “Indian GnRH Lyophilized Powder Reconstitution (Lupride Depot etc.)”Lupride Depot (leuprorelin) from India is commonly obtained in transgender communities due to its significantly lower cost compared to domestic equivalents. Lupride Depot comes as a lyophilized powder + diluent two-vial kit that requires reconstitution before injection.
Kit Contents:
- 1 vial of lyophilized powder (white powder containing leuprorelin 3.75 mg)
- 1 vial of diluent (sterile water for injection)
- Syringe and needles (included in some packages)
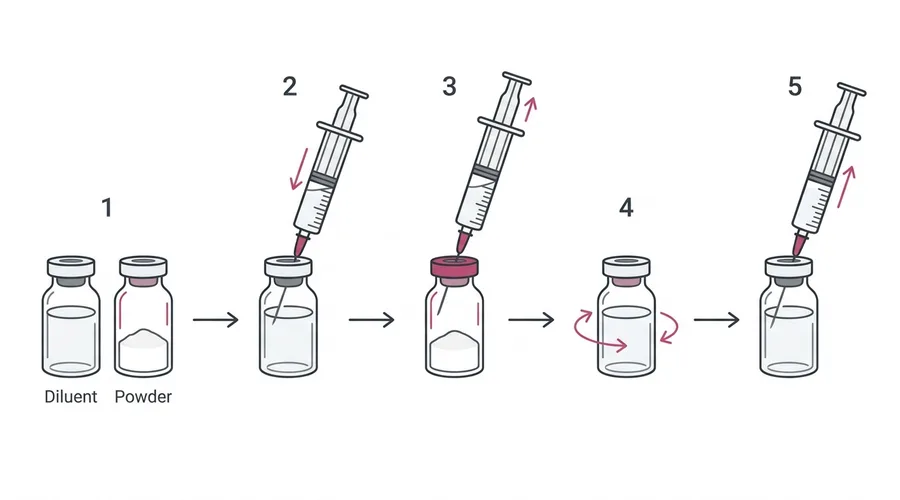
Reconstitution Steps:
- Inspect: Confirm both vials are within expiry date; powder should be white to off-white (no discoloration)
- Wash hands: Thoroughly wash hands with soap and water
- Disinfect: Swab both vial rubber stoppers with alcohol wipes, allow to air dry
- Draw diluent: Using a syringe with a drawing needle (18-20G), withdraw all diluent from the diluent vial
- Inject into powder vial: Slowly inject the diluent along the wall of the powder vial — do not spray directly onto the powder
- Dissolve: Gently swirl the vial (do not shake vigorously) until powder is fully dissolved. Solution should be clear or slightly opalescent
- Draw solution: Invert the vial and withdraw all reconstituted solution, expel air bubbles
- Change needle: Switch to injection needle (SC: 25-27G, IM: 21-23G)
- Inject: Follow the subcutaneous injection steps described above
Nasal Spray (Buserelin / Nafarelin)
Section titled “Nasal Spray (Buserelin / Nafarelin)”- Gently blow your nose to clear passages.
- Shake bottle and remove cap.
- Tilt head slightly forward; insert nozzle into one nostril.
- Press nozzle while inhaling gently.
- Alternate nostrils with each use.
- Avoid blowing your nose for 30 minutes after administration.
Implant (Histrelin)
Section titled “Implant (Histrelin)”The Supprelin LA implant is surgically placed under the skin of the inner upper arm by a healthcare provider. It continuously releases medication for 12 months, after which it must be surgically removed and replaced.
Storage Requirements
Section titled “Storage Requirements”| Drug | Storage | Notes |
|---|---|---|
| Leuprorelin (depot) | Room temperature (below 25°C) | Protect from light and heat |
| Goserelin (Zoladex) | Room temperature (below 25°C) | Pre-filled syringe; do not freeze |
| Triptorelin (Decapeptyl) | Refrigerate (2-8°C) | Lyophilized powder; reconstitute before use |
| Buserelin nasal spray | Room temperature | Use within 28 days of opening |
Flare Management
Section titled “Flare Management”The initial testosterone spike (“flare-up”) after the first GnRH agonist injection is a normal pharmacological response [1] .
Flare Timeline
Section titled “Flare Timeline”| Time | What Happens | Symptoms |
|---|---|---|
| Day 0 | GnRH agonist injected | — |
| Day 2-4 | T spikes to ~2× baseline | Possible acne, mood swings, libido changes |
| Day 7-8 | T returns to baseline | Symptoms begin to resolve |
| Day 14-28 | T drops to castrate level (< 50 ng/dL) | Full anti-androgen effect established |
How to Manage the Flare
Section titled “How to Manage the Flare”Missed Dose
Section titled “Missed Dose”- Missed injection: Administer as soon as possible (do not wait for the next scheduled date).
- Adjust schedule: Calculate the next dose from the actual injection date (monthly: +28 days; quarterly: +84 days).
- Delayed by >1 week: T may partially recover. Check T levels 4 weeks after the late injection.
- Missed nasal spray: Use as soon as remembered. Do not double the dose.
Side Effects
Section titled “Side Effects”Bone Density Loss
Section titled “Bone Density Loss”Long-term use without adequate estradiol can cause bone density decline [1] [2] :
- Both T and E2 are essential for bone maintenance
- Key: Maintaining E2 at 100-200 pg/mL substantially mitigates this risk
- DEXA scan recommended for users on GnRH agonists for > 2 years
Injection Site Reactions
Section titled “Injection Site Reactions”- Pain, redness, and induration at injection site (common)
- Goserelin’s 16G needle causes more pronounced discomfort
- Rotate injection sites to minimize reactions
Hot Flashes
Section titled “Hot Flashes”- Caused by rapid sex hormone suppression [2]
- Adequate estradiol dosing significantly reduces this
- Generally resolves once E2 levels stabilize
Mood Changes
Section titled “Mood Changes”- Some users experience mood fluctuations, especially early in treatment
- Generally milder than CPA’s mood effects
- Improves once hormone levels stabilize
Monitoring
Section titled “Monitoring”| Test | Frequency | Target / Alert | Action |
|---|---|---|---|
| Testosterone (T) | 4 weeks post-injection + every 3-6 months | T < 50 ng/dL | If high: assess injection interval/compliance |
| Estradiol (E2) | Tested with T | 100-200 pg/mL | Ensure adequate E2 for bone protection |
| Bone Density (DEXA) | Baseline + every 1-2 years after 2+ years | T-score > -1.0 | T-score < -2.5: osteoporosis — intervention needed |
| LH/FSH | Optional, first 3 months | LH < 1, FSH < 4.3 | Confirm pituitary suppression |
Blood draw timing: GnRH agonist depots maintain relatively stable drug levels. Blood can be drawn at any time relative to the injection — no specific timing window required.
GnRH Antagonists: Emerging Alternative
Section titled “GnRH Antagonists: Emerging Alternative”In addition to GnRH agonists, there are GnRH antagonists — drugs that directly block GnRH receptors without the initial flare.
| Drug | Brand | Mechanism | Time to Castrate | Advantage | Limitation |
|---|---|---|---|---|---|
| Degarelix | Firmagon | Direct GnRH receptor blockade | 3-7 days | No flare; faster onset | Monthly SubQ injection; prominent injection site reactions |
| Relugolix | Orgovyx | Oral GnRH antagonist | ~2 weeks | Oral administration; no flare | Daily oral dosing; very expensive; limited transgender evidence |
Advantages & Limitations
Section titled “Advantages & Limitations”Advantages
Section titled “Advantages”- Strongest, most reliable T suppression: Consistently achieves castrate levels [1]
- Excellent safety profile: No hepatotoxicity, no hyperkalemia, no meningioma risk
- Infrequent dosing: Monthly or quarterly injections; excellent compliance
- Reversible: HPG axis recovers after discontinuation (weeks to months); fertility can return
- Guideline-recommended: Endorsed by both ES 2017 and WPATH SOC 8 [2]
Limitations
Section titled “Limitations”- Prohibitive cost: $1,000-3,000/injection in the US; UK/EU NHS may cover; China ~¥1,000-2,000/month
- Injection required: Cannot be taken orally (nasal sprays have limited availability)
- Access barriers: Prescription required; often prescribed off-label for gender dysphoria
- Initial flare: First injection causes temporary T spike (manageable with anti-androgen cover)
- Bone density monitoring: Long-term use requires DEXA scans; must always co-administer estradiol
When to Consider GnRH Agonists
Section titled “When to Consider GnRH Agonists”- Finances allow sustained use
- CPA is contraindicated (liver issues, meningioma risk, severe mood effects)
- Spironolactone is intolerable (hyperkalemia risk, renal insufficiency)
- Maximum T suppression reliability is desired
- Adolescent puberty suppression (under specialist supervision)
May not be suitable when:
- Cost is prohibitive
- Regular clinic visits for injections are not feasible
- Severe osteoporosis is present (evaluate bone density first)
Brand Gallery
抑那通 / リュープリン (Lupron)
- Maker
- 武田 (Takeda) / AbbVie
- Spec
- 3.75mg / 11.25mg / 22.5mg 注射剂
- Form
- 预填充注射器,白色冻干粉末
日本最常用的 GnRH 激动剂,需皮下/肌肉注射,月剂型或季度剂型
贝依 / 抑那通
- Maker
- 丽珠集团 / AbbVie (中国)
- Spec
- 3.75mg / 11.25mg
- Form
- 注射用白色冻干粉末
中国大陆可获取的亮丙瑞林制剂,有国药准字批号,约 1000-2000 元/支
诺雷得 Zoladex
- Maker
- 阿斯利康 (AstraZeneca)
- Spec
- 3.6mg / 10.8mg 皮下植入剂
- Form
- 预填充注射器 + 固体缓释棒(16G 粗针)
皮下植入型 GnRH 激动剂,针头较粗,需医护操作。中国大陆有进口,有国药准字批号
达菲林 Decapeptyl
- Maker
- Ipsen
- Spec
- 3.75mg / 11.25mg / 22.5mg
- Form
- 注射用冻干粉末
法国产曲普瑞林,需肌肉注射。中国大陆有进口
Suprefact (布舍瑞林)
- Maker
- 赛诺菲 (Sanofi)
- Spec
- 鼻喷剂 100µg/喷 · 注射液
- Form
- 鼻喷瓶 / 注射液
唯一可用鼻喷剂型的 GnRH 激动剂,无需注射。每日 2-3 次喷鼻,全球供应有限
Supprelin LA (组氨瑞林)
- Maker
- Endo Pharmaceuticals
- Spec
- 65µg/天 × 12 个月皮下植入棒
- Form
- 小型柱状皮下植入棒
持续 12 个月的皮下植入棒,一年一次手术更换。价格极高(美国约 $45,000/年),主要用于青春期阻断