Oral vs Injectable Estradiol: Clinical Comparison of Routes
Oral estradiol (Progynova / estradiol valerate tablets) and intramuscular estradiol valerate (EV) injection are the two most common E2 routes in the Chinese-speaking MTF community. This page compares pharmacokinetics, safety, and practical barriers, without giving a universal recommendation.
At a Glance
Section titled “At a Glance”| Dimension | Oral (Progynova) | Injection (estradiol valerate, EV) |
|---|---|---|
| Hepatic first-pass | Yes (passes through) | No (bypassed) |
| VTE risk | 2-4x baseline | ~baseline |
| Dosing frequency | 1-3 times per day | Every 5-10 days |
| Plasma-level stability | Intra-day peaks/troughs | Inter-dose fluctuation |
| Onset | Hours to peak | Peaks in 24-48 hours |
| Evidence level | A | A |
| Availability in mainland China | Prescription-only; common in OB/GYN and endocrinology | Prescription-only; some hospitals reluctant to prescribe |
| Monthly cost | ~20-60 RMB | ~30-100 RMB |
| Practical barrier | Zero | Self-IM learning curve |
Pharmacokinetics
Section titled “Pharmacokinetics”Oral: hepatic first-pass shapes the curve
Section titled “Oral: hepatic first-pass shapes the curve”Oral estradiol or estradiol valerate is absorbed in the small intestine, enters the liver via the portal vein, and loses 50-70% to first-pass metabolism [13] . The systemic effective dose is only 30-50% of the swallowed dose, and the liver is “soaked” in high concentrations of E2/E1.
- Oral 2-4 mg → plasma peak ~50-150 pg/mL, falls back after 4-8 hours
- Half-life ~12-14 hours (as E2), but E1/E2 ratio is skewed high
- Hepatic production of SHBG, clotting factors, and CRP rises → elevated VTE / cholestasis risk [2]
Injection: muscular slow-release, flatter curve
Section titled “Injection: muscular slow-release, flatter curve”After IM EV injection, the oily vehicle forms a depot in the muscle and the ester bond hydrolyzes slowly to release E2 [1] :
- 4 mg EV IM → peaks 24-48 hours later at ~300-600 pg/mL, then declines exponentially
- Half-life ~4-5 days; falls to 100-150 pg/mL by 5-7 days
- Completely bypasses hepatic first-pass; coagulation effects approximate physiological estradiol
VTE Risk Comparison
Section titled “VTE Risk Comparison”Based on large MTF cohorts and postmenopausal HRT studies [2] [3] :
| Route | Relative VTE risk vs baseline |
|---|---|
| Oral estradiol | 2-4x |
| Conjugated equine estrogens (CEE, obsolete) | 4-6x |
| Sublingual | Possibly 1.5-3x (limited evidence) |
| Transdermal gel / patch | 1x (baseline) |
| IM estradiol valerate | 1x (baseline) |
Absolute risk is still low: baseline VTE in young, healthy MTF users is ~1-2/1000 person-years. Smoking + obesity + age >40 stack to substantially raise absolute risk.
- Age ≥40 + any risk factor → prefer non-oral
- History of VTE → avoid oral; prefer transdermal/injection + anticoagulation evaluation
- 2-4 weeks pre-surgery → switch to transdermal or pause
Plasma Stability
Section titled “Plasma Stability”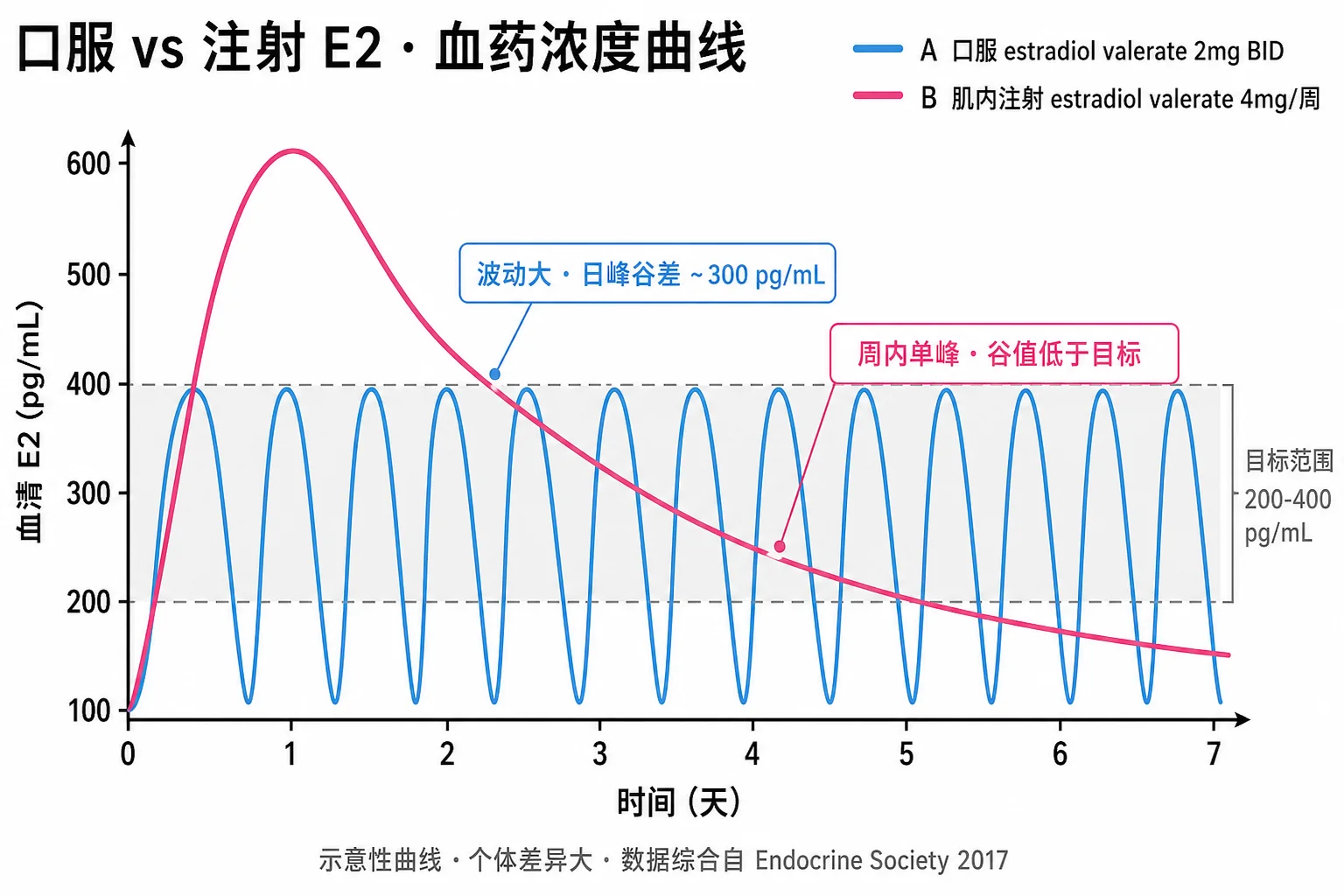
| Route | Intra-day variation | Inter-day variation | Symptom impact |
|---|---|---|---|
| Oral once daily | Peak/trough ~3:1 | Small | Mood swings · cyclical edema feeling |
| Oral twice daily | Peak/trough ~2:1 | Small | More even |
| Injection every 7 days | None | Peak/trough ~3-4:1 | ”Post-injection high” for a few days |
| Injection every 5 days | None | Peak/trough ~2:1 | Better steady state |
| Patch / gel | Small | Small | Most stable |
Selection logic: users seeking stable mood and embodiment prefer patch / gel / short-interval injection; users sensitive to dose flexibility prefer oral.
Onset and Switching
Section titled “Onset and Switching”Oral onset
Section titled “Oral onset”- Peak at 2-4 hours after dose; tissue responses (breast development, skin changes) appear at 1-3 months
- Steady-state T suppression ~4-8 weeks (with antiandrogen)
Injection onset
Section titled “Injection onset”- First injection peaks in 24-48 hours but cannot reach steady state
- After 2-3 doses (~10-20 days) approaches steady state
- During transition, overlap is recommended: keep oral going for 1-2 weeks before the first injection, then taper
Switching between routes
Section titled “Switching between routes”Oral → injection:
- Calculate equivalent dose: oral 2-4 mg/day ≈ EV 4-8 mg every 7 days
- Maintain oral for 2-4 days after the first injection, then taper
- Check trough E2 at 4-6 weeks post-injection to confirm steady state
Injection → oral:
- Stop the last injection; wait 5-7 days for plasma levels to fall
- Start oral; initial dose is often 1-1.5x the steady-state injection equivalent (to compensate for hepatic first-pass)
- Re-check bloodwork at 2-4 weeks for adjustment
Practical Barriers
Section titled “Practical Barriers”- Zero barrier; just take on schedule
- Note: Progynova is estradiol valerate 2 mg per tablet, equivalent to “estradiol 2 mg” — no conversion needed
- Missed dose: take it within 12 hours; skip if more than 12 hours late
Self-injection
Section titled “Self-injection”- Oily IM injection: 23G 1-1.5 inch needle (~25-38 mm), 21G for drawing
- Injection sites: dorsogluteal (upper outer quadrant), anterior lateral thigh, deltoid (small volumes)
- Disinfection: 70% alcohol; wipe vial stopper for 30 seconds, swab injection site in a circular motion
- Technique: bleed air bubbles, push slowly (10-30 seconds), press the site for 30 seconds after withdrawal
Subcutaneous (SC) alternative
Section titled “Subcutaneous (SC) alternative”Oily EV can be injected subcutaneously (abdomen, anterior thigh) with less pain and a slightly longer half-life. Needle 25G × 5/8 inch (16 mm). Evidence is moderate; some guidelines now accept it [1] .
Availability in Mainland China
Section titled “Availability in Mainland China”| Channel | Oral (Progynova) | Injection (EV) |
|---|---|---|
| OB/GYN | Stocked, easy to prescribe | Some hospitals decline |
| Endocrinology | Easy | Depends on physician attitude |
| Reproductive medicine | Very easy | Common in ovarian-stimulation protocols |
| Psychiatry (trans clinic) | Available | Available |
| Cost | 20 mg × 30 tabs ~40 RMB | 5 mg/mL × 10 amps ~60-100 RMB |
| Insurance | Partial reimbursement | Partial reimbursement |
How to Choose (Clinical Decision Framework)
Section titled “How to Choose (Clinical Decision Framework)”Prefer oral when:
- Young, no VTE risk factors, unwilling to learn IM injection
- Injection access is difficult or physicians refuse to prescribe
- Short-term bridge that will switch in a few months
- High acceptance of “daily medication” form
Prefer injection when:
- Age ≥40 or VTE risk factors (smoking/obesity/family history)
- Inconsistent oral absorption (GI surgery history, IBD)
- Seeking a flatter plasma profile
- Willing to learn self-injection
Prefer patch / gel (not compared on this page, but often optimal):
- VTE history or high risk
- Want to avoid needles entirely
- Sensitive to fine dose adjustment