유방 발달 - 서두르면 안 되는 이유
Why This Page Matters So Much
섹션 제목: “Why This Page Matters So Much”In many DIY and trans communities online, there is an abundance of misinformation floating around about breast growth—“the more you take, the faster they grow”, “I shot 10mg of EV and saw results in a week.” Not only do these claims lack scientific backing, they frequently result in permanent developmental impairment.
This page utilizes clinical evidence to demonstrate three things:
- The biological process of breast development
- Why high doses are counterproductive
- What regimen offers the best possible outcome
5.1 Normal Physiology - Tanner Stages
섹션 제목: “5.1 Normal Physiology - Tanner Stages”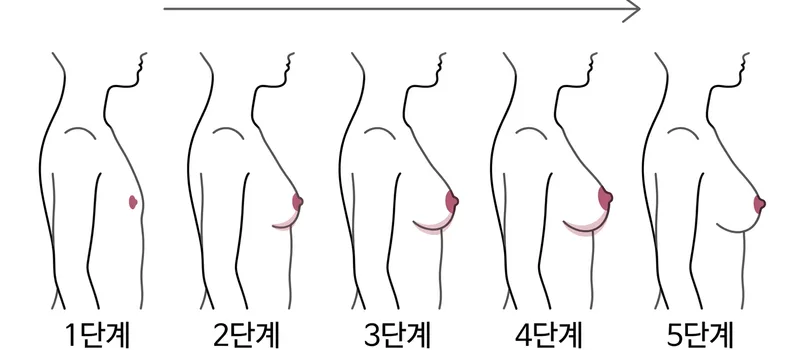
A Breast development follows the internationally recognized Tanner Staging System (Stages I-V), a process that typically runs for 3-5 years in cisgender women [3] .
| Stage | Characteristics | Typical Duration | Corresponding E2 Level |
|---|---|---|---|
| Tanner I | Pre-pubertal, no glandular tissue | — | < 20 pg/mL |
| Tanner II | Breast bud forms, small mound beneath areola | ~6-12 months | 20-60 pg/mL |
| Tanner III | Breast elevates beyond areolar perimeter, initial volume | ~6-12 months | 50-100 pg/mL |
| Tanner IV | Areola and papilla form a secondary mound | ~12-24 months | 100-200 pg/mL |
| Tanner V | Mature breast, areola recedes into the general contour | 12 months+ | 100-200 pg/mL |
Key Facts
섹션 제목: “Key Facts”- Cis female puberty starts with extremely low E2 levels—initially just 20-40 pg/mL [3]
- E2 levels escalate gradually, they do not jump to mature adult levels overnight
- Completing each Tanner Stage inherently requires adequate time, which cannot be circumvented by flooding the body with hormones
- This is a biological reality applicable to both cisgender and transgender women
5.2 Real-World Data for Transgender Women
섹션 제목: “5.2 Real-World Data for Transgender Women”B We have to confront the clinical reality: current data indicates that breast development in transgender women routinely falls short of expectations [4] [1] .
Large Cohort Study Data
섹션 제목: “Large Cohort Study Data”- de Blok 2018 Cohort (n=224): After 1 year of HRT, less than half reached an AAA cup, while only 3.6% exceeded an A cup [1]
- Patel 2021 Review: The majority of transgender women hit a plateau after 2-3 years of HRT, with most never reaching Tanner Stage V [5]
- Final breast volume strictly correlates with age of HRT onset, genetics (mother/sisters’ sizes), and body fat distribution [6]
What This Means For You
섹션 제목: “What This Means For You”The point of this data is not to crush your hopes, but to calibrate your expectations:
- Development is a multi-year process—month 12 does not equate to the final result
- Results are heavily influenced by genetics and age—not primarily by how high you crank your dose
- The poorest results frequently occur in individuals who initiated on exceptionally high doses early on—which leads directly into our next section
5.3 Why High Doses Backfire
섹션 제목: “5.3 Why High Doses Backfire”B This is the most critical section on this page. Read it carefully.
The Two Phases of Breast Development
섹션 제목: “The Two Phases of Breast Development”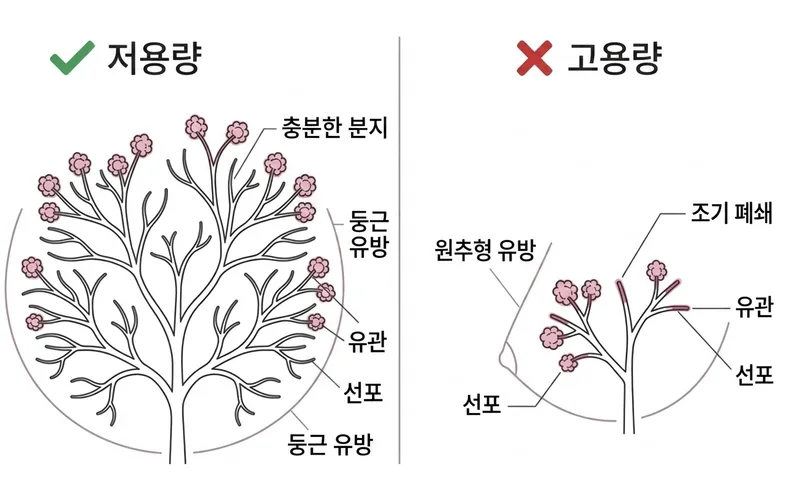
Breast development can be best understood through the analogy of a growing tree:
Phase One: Ductal Branching (Growing the Branches)
Triggered by low-to-moderate E2 levels, the ductal system proliferates and extends, much like a tree sprouting more and more branches [2] [7] . This process necessitates low E2 environments and ample time. The denser and wider the branching, the better the final breast volume and morphology will be.
Phase Two: Lobuloalveolar Maturation (Bearing Fruit)
Once the ductal framework is sufficiently established, higher E2 levels (and/or progesterone) trigger the duct ends to form alveoli (lobules)—similar to fruit budding on branches [1] [7] . This yields the plump volume and rounded shape of mature breasts.
How High Doses Wreck This Sequence
섹션 제목: “How High Doses Wreck This Sequence”Stating It Quantitatively
섹션 제목: “Stating It Quantitatively”| Approach | Initial E2 Levels | Likely Outcome |
|---|---|---|
| Low Dose Start (Recommended) | 50-100 pg/mL | Maximal ductal branching → Larger, rounder breasts |
| Moderate Dose Start | 100-200 pg/mL | Restricted ductal branching → Moderate development |
| High Dose Start (Dangerous) | > 200 pg/mL | Premature arrest → Small, dense, conical breasts |
| Mega Dose (e.g., 10mg/week injections) | > 500 pg/mL | Severe architectural damage → Hard plateau at Tanner III |
5.4 The Correct Stepped Approach
섹션 제목: “5.4 The Correct Stepped Approach”A International guidelines advocate for a regimen that mimics female puberty: initiating on a low dose and titrating up gradually corresponding to blood results [3] [6] .
E2 Target Roadmap
섹션 제목: “E2 Target Roadmap”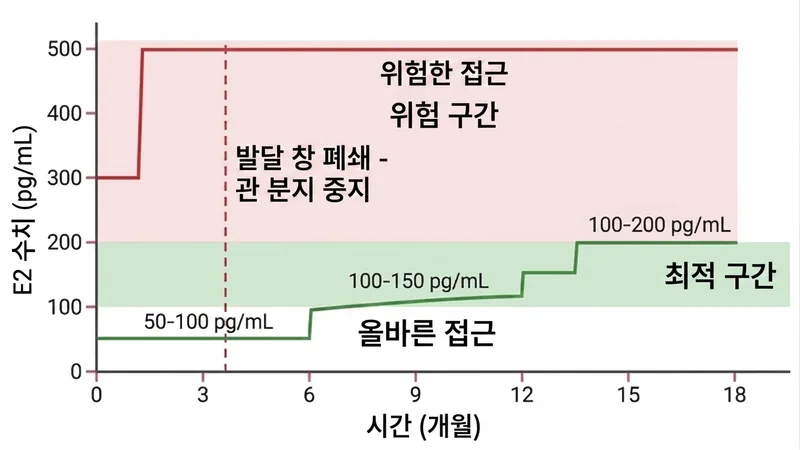
阶段 1: Initial Low Dose
Months 0-6Target E2: 50-100 pg/mL
The objective here is strictly to spur ductal branching. Do not panic-escalate the dose if “nothing seems to be happening” [3] [7] .
Baseline Dosages:
- Oral pills: 2 mg/day
- EV injections: 1-2 mg/week (Injection users must rigorously restrict this)
- Patches: 50-100 µg/day
Visible Changes: Sensitivity or mild nipple pain, softening skin—these are normal early indicators. Experiencing negligible physical shifts is also perfectly normal.
阶段 2: Moderate Titration
Months 6-12Target E2: 100-150 pg/mL
Ductal networking continues while visible breast mounding begins to materialize [3] [8] .
Baseline Dosages:
- Oral pills: 2-4 mg/day
- EV injections: 2-3 mg/week
- Patches: 100-200 µg/day
Guiding Principle: Let blood results dictate adjustments. If E2 is already in range, do not increase the dosage out of a desire for “faster” results.
阶段 3: Stable Maintenance
12 Months+Target E2: 100-200 pg/mL
Ductal branching is largely completed, and lobuloalveolar maturation hits its stride. Maintain this moderate E2 plateau. You may discuss introducing progesterone with your provider [3] [6] .
Baseline Dosages:
- Oral pills: 2-6 mg/day
- EV injections: 2-5 mg/week
- Patches: 100-200 µg/day
About Progesterone: Some anecdotal reports and studies suggest bioidentical micronized progesterone may improve sizing satisfaction. However, it should solely be introduced AFTER 12 months of HRT minimum [6] . Prematurely dumping progesterone into the mix can severely sabotage the branching phase.
Special Notice for Injection Users
섹션 제목: “Special Notice for Injection Users”E2 Level Roadmap Summary
섹션 제목: “E2 Level Roadmap Summary”| Phase | Timeline | E2 Target (pg/mL) | Injectable EV Example | Core Principle |
|---|---|---|---|---|
| Low Start | 0-6 Months | 50-100 | 1-2 mg/week | Prioritize ductal branching, do not rush |
| Moderate | 6-12 Months | 100-150 | 2-3 mg/week | Titrate using trough bloodwork |
| Maintenance | 12 Months+ | 100-200 | 2-5 mg/week | Use the minimum effective dose |
All dose modifications should be exclusively data-centric via bloodwork, not via emotional or subjective impatience. [3] [6]
5.5 Correcting Community Myths
섹션 제목: “5.5 Correcting Community Myths”X The following are pervasive myths circulated across trans communities that entirely lack scientific validity and frequently lead to self-harm.
| The Myth | The Reality | Source |
|---|---|---|
| "Take higher doses for faster growth" | Absolutely false. Cranking up E2 prematurely instigates terminal differentiation, ending the architectural branching process and culminating in substantially smaller final breasts. | Kanin 2025; Misakian 2025 |
| "My friend used 8mg day 1 and she looks great" | Survivorship bias. Those who irrevocably ruin their breast development don't post about their "spectacular failure." Plus, early "volume" is frequently just water retention/edema. | — |
| "Shot 10mg, breasts immediately swollen" | That is aggressive tissue edema/fluid retention induced by massive E2 toxicity, not genuine glandular development. It's likely harming long-term prospects. | Rothman 2024 |
| "Dark areolas mean it is working" | While minor darkening naturally occurs, significant areola hyperpigmentation within 3 months of starting HRT fundamentally points to excessive E2 causing premature terminal differentiation. | Poage 2026 |
| "Progesterone makes breasts huge and round" | While anecdotal evidence floats around, randomized controlled trials are absent. Most importantly, early introduction (before 12 months) directly sabotages branching. | Coleman 2022 |
| "My breasts are smaller than my cis age peers, I need more pills" | Breast morphology relies almost exclusively on body fat allocation and familial genetics. Tripling your dose won't augment your genetic baseline. | Hembree 2017 |
Why Are These Myths Prevalent?
섹션 제목: “Why Are These Myths Prevalent?”- Absence of Accessible Clinical Data: People turn to echo chambers instead of endocrinologists.
- Confirmation Bias: High-dose users experience edema (water weight) rapidly and mistakenly applaud it as effective results.
- Survivorship Bias: As discussed, the victims stay silent.
- Demand for Immediate Gratification: Waiting 3-5 years for a natural developmental progression is psychologically harrowing for practically everyone.
What If You Already Started On A Heavy Dose?
섹션 제목: “What If You Already Started On A Heavy Dose?”References
섹션 제목: “References”- Kanin M et al. (2025). Injectable Estradiol Dosing Regimens [1]
- Misakian AL et al. (2025). Injectable Estradiol Monotherapy in Transgender Individuals [2]
- Hembree WC et al. (2017). Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons [3]
- Aly (2021). Injectable Estradiol Meta-Analysis [4]
- Patel et al. (2021). Breast development in transgender women on hormone therapy [5]
- Coleman E et al. (2022). Standards of Care for the Health of Transgender and Gender Diverse People, Version 8 [6]
- Poage AC et al. (2026). Subcutaneous vs Intramuscular Estradiol Valerate Injection [7]
- Rothman MS et al. (2024). Injectable Estradiol Dosing in Transgender Individuals [8]