설하 에스트라디올
舌下含服雌二醇
Sublingual Estradiol
Sublingual
Sublingual administration involves dissolving standard oral estradiol pills under the tongue. This allows the medication to be absorbed directly through the mucosal membrane, partially bypassing first-pass liver metabolism. This vastly increases bioavailability but produces radical, rollercoaster-style fluctuations in blood levels, requiring users to dose multiple times per day.

Pharmacology
섹션 제목: “Pharmacology”The Absorption Mechanism
섹션 제목: “The Absorption Mechanism”When dissolved sublingually, estradiol enters the systemic circulation directly via the dense capillary network beneath the tongue [1] :
- Partially bypasses first-pass effect: Compared to swallowing pills, an enormously larger fraction of the drug sidesteps the liver’s direct metabolic destruction.
- Higher Bioavailability: Sublingual bioavailability is approximately 2 to 5 times greater than that of oral routes [2] .
- Rapid Onset: Blood concentrations start to skyrocket within 15 to 25 minutes of administration.
- Not a Complete Bypass: Saliva will inevitably carry some dissolved drug down your throat during the process, meaning a percentage of the dose will still be processed identically to an oral dose.
Blood Concentration Profiles (The Rollercoaster)
섹션 제목: “Blood Concentration Profiles (The Rollercoaster)”Sublingual pharmacokinetics differ radically from standard oral delivery [1] :
| Parameter | Sublingual | Oral |
|---|---|---|
| Time to Peak (Tmax) | ~0.5 to 1 hour | ~3 to 6 hours |
| Peak Concentration (Cmax) | Very High (~2-5x oral levels) | Relatively Low |
| Duration of Elevated Levels | Short (~4-6 hours before crashing) | Longer (~8-12 hours) |
| Intraday Fluctuation | Massive (high peak-to-trough ratio) | Moderate |
| E1/E2 Ratio | Lower (Favorable) | Higher |
The E1/E2 Ratio Advantage
섹션 제목: “The E1/E2 Ratio Advantage”A theoretical advantage to sublingual administration is maintaining a lower ratio of E1 (Estrone) to E2 (Estradiol) [2] :
- When swallowing pills, the liver rapidly converts E2 into E1 (a weakly active estrogen), resulting in an E1/E2 ratio of 5:1 or even higher.
- Because sublingual bypasses the liver significantly, the E1/E2 ratio stays much closer to 1:1.
- Because E2 drives the vast majority of feminization, a heavier E2 bias is theoretically superior.
- However, the clinical community lacks robust data confirming that manipulating the E1/E2 ratio yields a superior final phenotypic outcome.
Dosage Recommendations
섹션 제목: “Dosage Recommendations”Due to the aggressively heightened bioavailability, the effective sublingual dose is technically lower than the equivalent oral dose [3] :
Conversion Estimate
섹션 제목: “Conversion Estimate”Because sublingual hits your bloodstream at 2x to 5x the strength of swallowed pills, rough community consensus often estimates:
1 mg Sublingual ≈ 2-3 mg Oral (rough equivalence)
Keep in mind, individual metabolic clearance rates vary wildly.
Recommended Dosing
섹션 제목: “Recommended Dosing”| Stage | Sublingual Dose | Frequency | Target Trough E2 (pg/mL) | Timeline |
|---|---|---|---|---|
| Low Dose Start | 0.5-1 mg/dose | Twice a day | 50-100 | Months 1-6 |
| Moderate Titration | 1-2 mg/dose | 2 to 3 times a day | 100-200 | Months 6-12 |
| Maintenance Phase | 1-2 mg/dose | 2 to 3 times a day | 100-200 | 12 Months+ |
| Typical Maximum | 2 mg/dose | 3 times a day (Total 6mg) | Not to exceed 200 | Special circumstances |
How to Take It
섹션 제목: “How to Take It”Technique
섹션 제목: “Technique”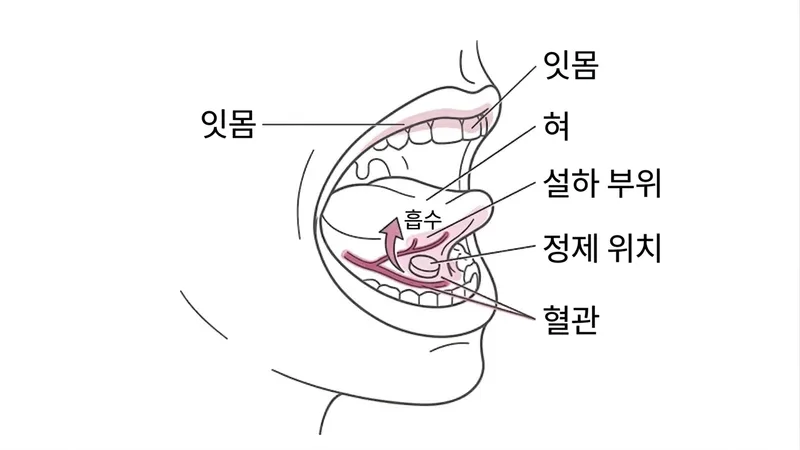
- Place the pill completely under the tongue (nestled close to the gums/veins).
- Keep your mouth closed and actively avoid swallowing your saliva.
- Let it dissolve naturally. With micronized pills like Estrofem, this takes roughly 5-15 minutes.
- Do not talk, drink, or eat during this window.
- After it has entirely disintegrated, wait another 1-2 minutes, then swallow whatever saliva remains naturally.
FAQ
섹션 제목: “FAQ”- The pill won’t break down? Some pill formulations (especially thick sugar-coated Progynova Valerate pills depending on the manufacturer) are difficult to dissolve sublingually. Micronized Estradiol Hemihydrate (like Estrofem) crushes and dissolves almost instantaneously.
- Accidentally swallowed it early? Just treat it as a swallowed oral dose. Do not take another one to “make up for it.”
- Producing too much saliva? This is normal. Resist swallowing actively, but don’t panic if you swallow a bit—your sublingual mucosa absorbs incredibly quickly.
Target Audience
섹션 제목: “Target Audience”Sublingual dosing is a strong fit for individuals who:
- Want higher bioavailability than swallowing pills, but have zero access to transdermal options.
- Are specifically trying to drive down high estrone (E1) levels.
- Possess the strict discipline to dose 3 times a day perfectly.
It is a terrible fit if you:
- Struggle with compliance or remembering to take medications.
- Cannot handle emotional instability or energy crashes associated with spiking hormones.
- Have a history of VTE and have access to patches/gel.
VTE (Clotting) Risk
섹션 제목: “VTE (Clotting) Risk”There is a frustrating lack of large-scale clinical data mapping VTE risk specifically to sublingual dosing [4] :
- In theory: Bypassing the liver implies a reduced impact on coagulation factors, making it theoretically safer than oral.
- In reality: You always swallow some of the dose in your saliva, preventing a true and total liver bypass. Therefore, real-world VTE risk likely sits uncomfortably between transdermal and oral.
- The Verdict: Do not use sublingual as a “loophole” if you have preexisting blood clot risks. If you are high risk, demand transdermal administration [3] .
Comparison Quick Reference
섹션 제목: “Comparison Quick Reference”| Metric | Sublingual | Oral (Swallowed) | Transdermal Patch |
|---|---|---|---|
| Bioavailability | Moderate-to-High | Low (~5%) | High |
| Blood Level Stability | Terrible (Massive peaks) | Moderate | Excellent (Extremely stable) |
| VTE Risk | Likely falls somewhere in the middle | RR ≈ 1.48 | RR ≈ 0.97 |
| Dosing Frequency | 2-3 times daily | 1-2 times daily | Once every 3.5-7 days |
| Convenience | Low | High | High |
品牌图鉴
Estrofem
- 厂商
- Novo Nordisk
- 规格
- 2mg × 28片
- 外观
- 蓝色三角形薄膜衣片
最常用于舌下含服的制剂,微粉化雌二醇
补佳乐 Progynova
- 厂商
- 拜耳 / Zydus
- 规格
- 1mg / 2mg
- 外观
- 糖衣片
可舌下含服但非官方适应症,糖衣影响含服速度