GnRH 작용제
GnRH Agonists (GnRH 激动剂)
GnRH Agonists (Leuprorelin, Goserelin, Triptorelin, etc.)
Subcutaneous / Intramuscular Injection · Nasal Spray · Implant
GnRH Agonists are the most effective anti-androgen available, suppressing testosterone to castrate levels (< 50 ng/dL) by shutting down the hypothalamic-pituitary-gonadal axis. Both the Endocrine Society 2017 and WPATH SOC 8 recommend their use. When accessible, GnRH agonists are the ideal anti-androgen choice.
Pharmacology
섹션 제목: “Pharmacology”How They Work
섹션 제목: “How They Work”GnRH agonists act at a fundamentally different level than other anti-androgens — they target the upstream control center of hormone production [1] :
- Flare-Up Phase: For the first 1-2 weeks, the drug overstimulates pituitary GnRH receptors, causing a transient spike in LH/FSH and testosterone.
- Receptor Desensitization: Continuous stimulation causes pituitary GnRH receptors to downregulate and become unresponsive.
- Total Suppression: Within 2-4 weeks, LH/FSH output ceases, dropping T to castrate levels (< 50 ng/dL).
This mechanism suppresses T directly and reliably — without the hepatotoxicity risk of CPA or the hyperkalemia risk of spironolactone [2] .
T Suppression Compared to Other Anti-Androgens
섹션 제목: “T Suppression Compared to Other Anti-Androgens”| Anti-Androgen | Mechanism | T Suppression | Main Limitation |
|---|---|---|---|
| GnRH Agonists | HPG axis shutdown | ~95% (< 50 ng/dL) | Extremely expensive; injection required |
| CPA 5-12.5mg | AR antagonism + progestogenic feedback | ~90% (female range) | Meningioma risk (≥25mg) |
| Spironolactone 100-200mg | Weak AR antagonism | ~30-50% (often insufficient) | Hyperkalemia; unreliable T suppression |
| Bicalutamide 50mg | Pure AR antagonism | T may increase | Hepatotoxicity; requires monitoring |
Available Formulations
섹션 제목: “Available Formulations”Injectable Forms
섹션 제목: “Injectable Forms”| Drug | Brand Names | Dose | Interval | Route | Self-Administration |
|---|---|---|---|---|---|
| Leuprorelin | Lupron / Eligard / Prostap | 3.75mg / 11.25mg / 22.5mg / 45mg | Monthly / 3-month / 6-month | SubQ or IM | Some SubQ forms can be self-injected |
| Goserelin | Zoladex | 3.6mg / 10.8mg | Monthly / 3-month | SubQ implant (abdomen) | Requires clinical administration (16G needle) |
| Triptorelin | Decapeptyl / Trelstar | 3.75mg / 11.25mg / 22.5mg | Monthly / 3-month / 6-month | IM injection | Requires clinical administration |
Non-Injectable Forms
섹션 제목: “Non-Injectable Forms”| Drug | Brand | Form | Administration | Advantage | Limitation |
|---|---|---|---|---|---|
| Buserelin | Suprefact | Nasal spray | 2-3 sprays daily | No injection needed | Compliance burden (multiple daily doses) |
| Nafarelin | Synarel | Nasal spray | 2-3 sprays daily | Non-invasive; ~95% T reduction | Limited global supply |
| Histrelin | Supprelin LA | SubQ implant rod | Surgical insertion in upper arm; lasts 12 months | Once-yearly; best compliance | Very expensive; requires surgical insertion/removal |
Administration Guide
섹션 제목: “Administration Guide”Subcutaneous Injection (Leuprorelin, etc.)
섹션 제목: “Subcutaneous Injection (Leuprorelin, etc.)”Most GnRH agonists are administered via subcutaneous or intramuscular injection. Some formulations (e.g., leuprorelin SubQ) can be self-administered after nurse training [1] .
Injection Site Selection:
- Primary: Abdomen, approximately 5cm lateral to the navel (avoid 2cm around navel)
- Alternative: Anterior outer thigh, mid-section
- Rotation: Alternate sites each injection; maintain at least 3cm between injection points; avoid areas with lumps or bruising
Subcutaneous Injection Steps:
- Prepare: Wash hands. Bring refrigerated medication to room temperature (15-30 minutes). Check expiry date and solution appearance.
- Clean: Swab injection site with alcohol prep pad. Allow to air-dry completely.
- Pinch: Using your non-dominant hand, pinch a 2cm fold of skin.
- Insert: Insert needle at 45-90° angle quickly and firmly, burying the needle fully (1-2cm depth).
- Inject: Depress plunger slowly over ~30 seconds. Do not rush.
- Withdraw: Release skin, then withdraw needle swiftly. Press dry cotton ball on site for 15 seconds (do not rub).
- Dispose: Place needle in sharps container. Record date and injection site.
인도산 GnRH 동결건조분말 조제 (Lupride Depot 등)
섹션 제목: “인도산 GnRH 동결건조분말 조제 (Lupride Depot 등)”인도산 Lupride Depot(류프로렐린)은 국내 동등 제품보다 훨씬 저렴하여 트랜스젠더 커뮤니티에서 널리 구입되고 있습니다. Lupride Depot은 동결건조분말 + 용매 2바이알 키트로, 주사 전에 직접 조제(용해)해야 합니다.
키트 구성:
- 동결건조분말 바이알 1개 (백색 분말, 류프로렐린 3.75 mg 함유)
- 용매 바이알 1개 (멸균 주사용수)
- 주사기 및 바늘 (일부 포장에 포함)
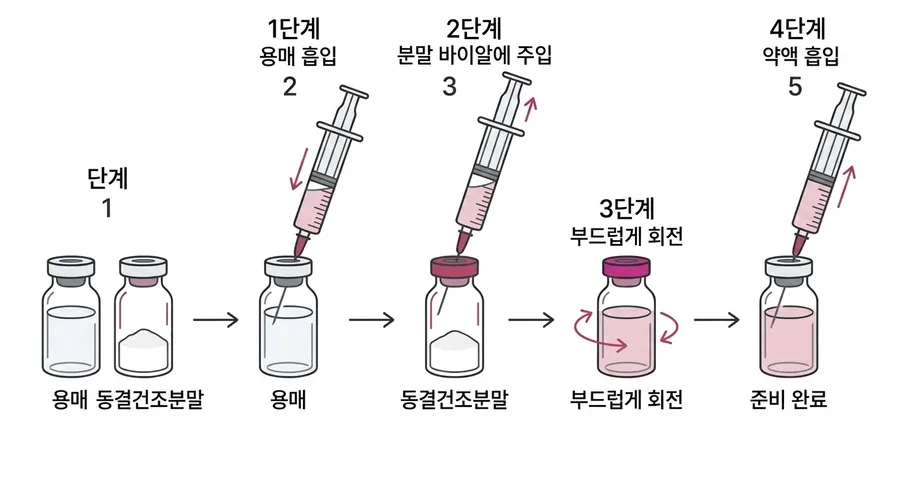
조제(용해) 절차:
- 확인: 두 바이알 모두 유효기간 내인지, 분말이 백색~유백색인지(변색 없는지) 확인
- 손 씻기: 비누와 물로 손을 철저히 씻기
- 소독: 두 바이알의 고무 마개를 알코올 솜으로 닦고 자연 건조
- 용매 흡입: 주사기(굵은 바늘 18-20G)로 용매 바이알에서 전량 흡입
- 분말 바이알에 주입: 용매를 분말 바이알 벽면을 따라 천천히 주입 — 분말에 직접 분사하지 말 것
- 용해: 바이알을 부드럽게 회전 (격렬하게 흔들지 말 것). 분말이 완전히 녹을 때까지 기다림. 용액은 투명하거나 약간 유백색
- 약액 흡입: 바이알을 뒤집어 조제된 약액 전량을 흡입하고 기포 제거
- 바늘 교체: 주사용 바늘로 교체 (SC: 25-27G, IM: 21-23G)
- 주사: 위의 피하주사 절차에 따라 시행
Nasal Spray (Buserelin / Nafarelin)
섹션 제목: “Nasal Spray (Buserelin / Nafarelin)”- Gently blow your nose to clear passages.
- Shake bottle and remove cap.
- Tilt head slightly forward; insert nozzle into one nostril.
- Press nozzle while inhaling gently.
- Alternate nostrils with each use.
- Avoid blowing your nose for 30 minutes after administration.
Implant (Histrelin)
섹션 제목: “Implant (Histrelin)”The Supprelin LA implant is surgically placed under the skin of the inner upper arm by a healthcare provider. It continuously releases medication for 12 months, after which it must be surgically removed and replaced.
Storage Requirements
섹션 제목: “Storage Requirements”| Drug | Storage | Notes |
|---|---|---|
| Leuprorelin (depot) | Room temperature (below 25°C) | Protect from light and heat |
| Goserelin (Zoladex) | Room temperature (below 25°C) | Pre-filled syringe; do not freeze |
| Triptorelin (Decapeptyl) | Refrigerate (2-8°C) | Lyophilized powder; reconstitute before use |
| Buserelin nasal spray | Room temperature | Use within 28 days of opening |
Flare Management
섹션 제목: “Flare Management”The initial testosterone spike (“flare-up”) after the first GnRH agonist injection is a normal pharmacological response [1] .
Flare Timeline
섹션 제목: “Flare Timeline”| Time | What Happens | Symptoms |
|---|---|---|
| Day 0 | GnRH agonist injected | — |
| Day 2-4 | T spikes to ~2× baseline | Possible acne, mood swings, libido changes |
| Day 7-8 | T returns to baseline | Symptoms begin to resolve |
| Day 14-28 | T drops to castrate level (< 50 ng/dL) | Full anti-androgen effect established |
How to Manage the Flare
섹션 제목: “How to Manage the Flare”Missed Dose
섹션 제목: “Missed Dose”- Missed injection: Administer as soon as possible (do not wait for the next scheduled date).
- Adjust schedule: Calculate the next dose from the actual injection date (monthly: +28 days; quarterly: +84 days).
- Delayed by >1 week: T may partially recover. Check T levels 4 weeks after the late injection.
- Missed nasal spray: Use as soon as remembered. Do not double the dose.
Side Effects
섹션 제목: “Side Effects”Bone Density Loss
섹션 제목: “Bone Density Loss”Long-term use without adequate estradiol can cause bone density decline [1] [2] :
- Both T and E2 are essential for bone maintenance
- Key: Maintaining E2 at 100-200 pg/mL substantially mitigates this risk
- DEXA scan recommended for users on GnRH agonists for > 2 years
Injection Site Reactions
섹션 제목: “Injection Site Reactions”- Pain, redness, and induration at injection site (common)
- Goserelin’s 16G needle causes more pronounced discomfort
- Rotate injection sites to minimize reactions
Hot Flashes
섹션 제목: “Hot Flashes”- Caused by rapid sex hormone suppression [2]
- Adequate estradiol dosing significantly reduces this
- Generally resolves once E2 levels stabilize
Mood Changes
섹션 제목: “Mood Changes”- Some users experience mood fluctuations, especially early in treatment
- Generally milder than CPA’s mood effects
- Improves once hormone levels stabilize
Monitoring
섹션 제목: “Monitoring”| Test | Frequency | Target / Alert | Action |
|---|---|---|---|
| Testosterone (T) | 4 weeks post-injection + every 3-6 months | T < 50 ng/dL | If high: assess injection interval/compliance |
| Estradiol (E2) | Tested with T | 100-200 pg/mL | Ensure adequate E2 for bone protection |
| Bone Density (DEXA) | Baseline + every 1-2 years after 2+ years | T-score > -1.0 | T-score < -2.5: osteoporosis — intervention needed |
| LH/FSH | Optional, first 3 months | LH < 1, FSH < 4.3 | Confirm pituitary suppression |
Blood draw timing: GnRH agonist depots maintain relatively stable drug levels. Blood can be drawn at any time relative to the injection — no specific timing window required.
GnRH Antagonists: Emerging Alternative
섹션 제목: “GnRH Antagonists: Emerging Alternative”In addition to GnRH agonists, there are GnRH antagonists — drugs that directly block GnRH receptors without the initial flare.
| Drug | Brand | Mechanism | Time to Castrate | Advantage | Limitation |
|---|---|---|---|---|---|
| Degarelix | Firmagon | Direct GnRH receptor blockade | 3-7 days | No flare; faster onset | Monthly SubQ injection; prominent injection site reactions |
| Relugolix | Orgovyx | Oral GnRH antagonist | ~2 weeks | Oral administration; no flare | Daily oral dosing; very expensive; limited transgender evidence |
Advantages & Limitations
섹션 제목: “Advantages & Limitations”Advantages
섹션 제목: “Advantages”- Strongest, most reliable T suppression: Consistently achieves castrate levels [1]
- Excellent safety profile: No hepatotoxicity, no hyperkalemia, no meningioma risk
- Infrequent dosing: Monthly or quarterly injections; excellent compliance
- Reversible: HPG axis recovers after discontinuation (weeks to months); fertility can return
- Guideline-recommended: Endorsed by both ES 2017 and WPATH SOC 8 [2]
Limitations
섹션 제목: “Limitations”- Prohibitive cost: $1,000-3,000/injection in the US; UK/EU NHS may cover; China ~¥1,000-2,000/month
- Injection required: Cannot be taken orally (nasal sprays have limited availability)
- Access barriers: Prescription required; often prescribed off-label for gender dysphoria
- Initial flare: First injection causes temporary T spike (manageable with anti-androgen cover)
- Bone density monitoring: Long-term use requires DEXA scans; must always co-administer estradiol
When to Consider GnRH Agonists
섹션 제목: “When to Consider GnRH Agonists”- Finances allow sustained use
- CPA is contraindicated (liver issues, meningioma risk, severe mood effects)
- Spironolactone is intolerable (hyperkalemia risk, renal insufficiency)
- Maximum T suppression reliability is desired
- Adolescent puberty suppression (under specialist supervision)
May not be suitable when:
- Cost is prohibitive
- Regular clinic visits for injections are not feasible
- Severe osteoporosis is present (evaluate bone density first)
品牌图鉴
抑那通 / リュープリン (Lupron)
- 厂商
- 武田 (Takeda) / AbbVie
- 规格
- 3.75mg / 11.25mg / 22.5mg 注射剂
- 外观
- 预填充注射器,白色冻干粉末
日本最常用的 GnRH 激动剂,需皮下/肌肉注射,月剂型或季度剂型
贝依 / 抑那通
- 厂商
- 丽珠集团 / AbbVie (中国)
- 规格
- 3.75mg / 11.25mg
- 外观
- 注射用白色冻干粉末
中国大陆可获取的亮丙瑞林制剂,有国药准字批号,约 1000-2000 元/支
诺雷得 Zoladex
- 厂商
- 阿斯利康 (AstraZeneca)
- 规格
- 3.6mg / 10.8mg 皮下植入剂
- 外观
- 预填充注射器 + 固体缓释棒(16G 粗针)
皮下植入型 GnRH 激动剂,针头较粗,需医护操作。中国大陆有进口,有国药准字批号
达菲林 Decapeptyl
- 厂商
- Ipsen
- 规格
- 3.75mg / 11.25mg / 22.5mg
- 外观
- 注射用冻干粉末
法国产曲普瑞林,需肌肉注射。中国大陆有进口
Suprefact (布舍瑞林)
- 厂商
- 赛诺菲 (Sanofi)
- 规格
- 鼻喷剂 100µg/喷 · 注射液
- 外观
- 鼻喷瓶 / 注射液
唯一可用鼻喷剂型的 GnRH 激动剂,无需注射。每日 2-3 次喷鼻,全球供应有限
Supprelin LA (组氨瑞林)
- 厂商
- Endo Pharmaceuticals
- 规格
- 65µg/天 × 12 个月皮下植入棒
- 外观
- 小型柱状皮下植入棒
持续 12 个月的皮下植入棒,一年一次手术更换。价格极高(美国约 $45,000/年),主要用于青春期阻断