HRT 임상 경로
This pathway is based on WPATH SOC 8 [1] and Endocrine Society 2017 [2] , providing a standardized framework for transfeminine HRT initiation and maintenance.
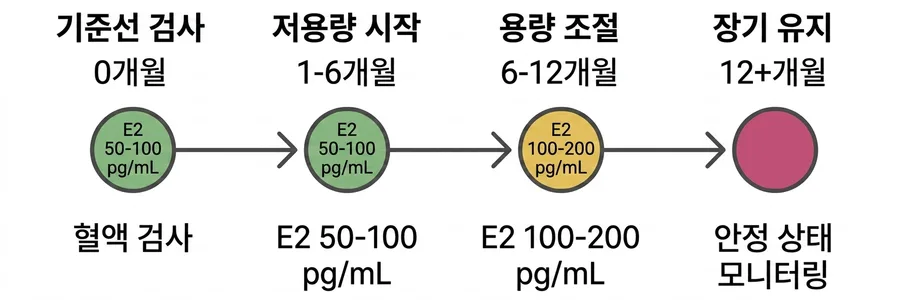
阶段 0: Baseline Assessment
Before starting any medication, complete a full baseline panel to rule out contraindications and establish your personal reference values.
Sex hormones (E2, T, SHBG, LH/FSH)
Hepatic & renal function, lipid panel
Coagulation panel & D-dimer
Fasting glucose + CBC
阶段 1: Low-Dose Initiation
1-6 MONTHS| Route | Starting Dose | Source |
|---|---|---|
| Oral estradiol | 2.0 mg / day | [2] |
| Transdermal patch | 50-100 µg / 24h | [2] |
| Topical gel | 1.5 mg / day | [2] |
| IM estradiol valerate | 1-2 mg / week | [3] |
Anti-androgen (if needed): CPA 5-12.5 mg/day or spironolactone 50-100 mg/day. [2] = Hembree et al. 2017 [2] ; [3] = Rothman 2024 [3]
Target E2
50-100 pg/mL
Target T Trend
↓ Declining
Safety warning: Your body needs time to adapt to receptor changes. Never increase dose without blood work. Do not escalate even if you feel “nothing is happening.” Breast bud signals typically appear at 3-6 months.
3 MONTH
DECISION
阶段 2: Dose Titration
6-12 MONTHSAdjust based on 3-month lab results. The goal is to reach the standard physiologic range for transfeminine individuals.
| Route | Adjusted Dose |
|---|---|
| Transdermal patch | 100-200 µg / day |
| Oral estradiol | 4 mg / day |
| Topical gel | 3 mg / day |
| IM estradiol valerate | 2-4 mg / week |
Target E2
100-200 pg/mL
Target T
<50 ng/dL
Progesterone (optional)
Consider based on breast development (Tanner 3+)
6 MONTH
STABILITY
阶段 3: Long-Term Maintenance
12 MONTHS+Once levels and physical changes stabilize, transition to low-frequency monitoring. Maintain the minimum effective dose to keep E2 100-200 pg/mL, T <50 ng/dL.
Monitoring Frequency
6
Months
Full hormone panel and VTE risk factors every 6 months. Annual lipids and fasting glucose. Consider bone density screening.
E2 >200 pg/mL does not produce more feminization — it only increases risk (Endocrine Society 2017, Rec 2.2)
END OF INITIAL PHASE
Ongoing Monitoring